

I’ve been asked this question more times than I can count, usually by someone who just got a look from a coworker or noticed white flakes on a black shirt. The question behind the question is always the same: Is this a real problem, or am I just bad at showering?
Short answer: yes, dandruff is a real medical condition. I say that as someone who has it, who has read a lot of the research, and who has spent more money on medicated shampoos than I care to admit.
Let me walk you through why.
What “disease” actually means here
When most people hear “disease” they picture something contagious or serious. Dandruff is neither; but that doesn’t mean it isn’t a genuine condition with a known cause and real physical effects.
The classic medical definition of disease covers any process that disrupts normal body function and produces recognizable signs or symptoms. Dandruff checks that box. There’s a mechanism, there are symptoms (flaking, sometimes itching, sometimes redness), and for a meaningful percentage of people it’s persistent and recurring. That’s not nothing.
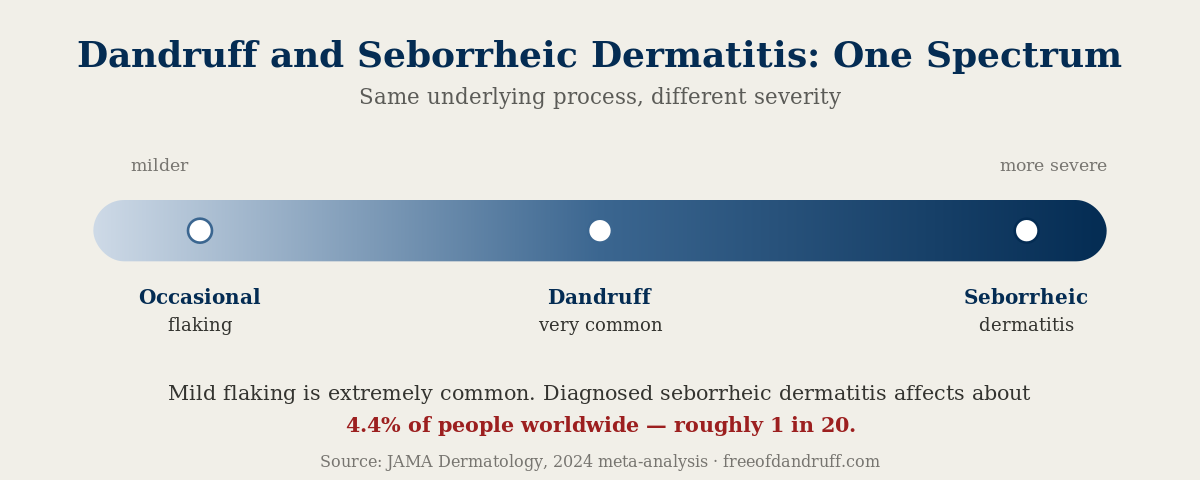
The bigger picture, though, is that modern dermatology doesn’t really treat dandruff as a completely separate thing from [seborrheic dermatitis](link: what is seborrheic dermatitis -> /what-is-dandruff/). They sit on a spectrum. Dandruff is the mild, non-inflammatory end: flaking without much redness. Seborrheic dermatitis (SD) is the more inflamed version: greasy yellowish scales, irritated skin, sometimes spreading to the face, ears, or chest. Same root cause, different severity. Understanding that spectrum is actually what convinced me I wasn’t being dramatic about my own scalp.
The three-factor model: why you have it and your roommate doesn’t
Here’s where it gets interesting. For a long time, the explanation was basically “oily scalp = dandruff.” That’s not wrong, but it misses most of the story.
The current model has three factors working together: you need all three for dandruff to develop:
1. Malassezia yeast
There’s a fungus living on your scalp. On everyone’s scalp. That’s normal. The species most directly linked to dandruff are Malassezia globosa and M. restricta; that understanding came from whole-genome analysis work published in the Journal of Investigative Dermatology Symposium Proceedings, which I’ll link in the references. Earlier research had blamed a different species (M. furfur), so the science has actually moved on this.
2. Sebum
Malassezia feeds on sebum: the oil your scalp produces naturally. It puts out enzymes called lipases that break sebum’s fats (triglycerides) into free fatty acids. The yeast consumes the saturated ones for nutrition. What it leaves behind is oleic acid, and that’s where things go sideways.
3. Individual susceptibility
This is the part that explains the roommate situation. In people with a predisposed skin barrier, oleic acid penetrates the scalp and triggers irritation, inflammation, and the rapid cell turnover that produces visible flakes. In people without that susceptibility, the same yeast and the same oleic acid just… sit there without causing a problem.
The barrier dysfunction and the downstream immune response (toll-like receptors lighting up, keratinocytes misfiring) are where the actual disease process lives. It’s not about hygiene. It’s not about being dirty. It’s a combination of your personal biology and this ubiquitous yeast doing what it does. learn more about the causes
I’ll be honest, learning this actually made me feel better. I’d been blaming myself for years.
How common is this (really)
Old articles (including earlier versions of this one) cited that figure about half the world’s population having dandruff. Let me update that with something more precise.
A 2024 systematic review and meta-analysis published in JAMA Dermatology analyzed 121 studies covering 1,260,163 people across nine countries. The pooled global prevalence for clinically diagnosed seborrheic dermatitis came out at 4.38%: about 5.64% in adults, 3.70% in children. The U.S. rate was 5.86%. South Africa was highest at 8.82%. India lowest at 2.62%.
Separate burden-of-disease analysis found approximately 135.7 million people had SD globally in 2021: a 53% increase since 1990, though researchers believe that reflects population growth and better detection rather than a true explosion in cases.
Now, those numbers are for diagnosed seborrheic dermatitis, the more inflammatory form. Milder dandruff (the kind where you mostly just have flaking without a formal diagnosis) is far more common. Many people deal with some level of scalp flaking at some point in their lives and never see a dermatologist about it. So the “almost half of adults” figure that circulates online is probably closer to the truth for dandruff in the broader sense, even if clinical SD is closer to 4-6%.
The point is: whichever end of the spectrum you’re on, you’re not alone, and it’s not imaginary.
Why “it’s just dry skin” is wrong
A lot of people (including past me) assume dandruff is a dry scalp problem. That’s actually the opposite of what’s happening. Dandruff is associated with excess sebum production. The Malassezia yeast thrives in that oily environment. Dry scalp (small, powdery flakes, tight-feeling skin, no real itch) is a different animal with a different fix.
dandruff vs dry scalp is worth reading if you’re not sure which one you’re dealing with. Treating dry scalp with an anti-fungal shampoo isn’t going to help much.
The seborrheic dermatitis spectrum
If your dandruff is more than mild (if there’s redness, the flakes are yellowish and greasy, if it’s showing up on your eyebrows or around your nose) you might be further along the spectrum toward SD. That’s worth seeing a dermatologist about, partly because the treatments are similar but may need to be stronger (prescription ketoconazole rather than OTC Head & Shoulders), and partly because SD can sometimes look like other conditions. dandruff vs psoriasis is a real distinction that matters for treatment.
I want to be clear: I’m not diagnosing anyone here. I’m just a guy who did a lot of reading. If your scalp is persistently inflamed or you’ve tried OTC options without results, please talk to an actual dermatologist.
So yes: it qualifies as a disease
Not in the dramatic sense. It won’t kill you. It’s not contagious. Permanent hair loss isn’t a standard outcome. But it is a chronic condition with:
- A known, multi-factor cause (Malassezia + sebum + individual susceptibility/barrier dysfunction)
- A clear physical mechanism (oleic acid irritating a compromised skin barrier)
- Documented symptoms (flaking, itching, inflammation)
- Real prevalence data showing it affects tens of millions of people
- Evidence-based treatments that actually work: not just for cosmetic reasons, but because the underlying process responds to them
how Malassezia actually causes flaking
The reason this classification matters is practical. If it’s a real condition with a real cause, then there are real interventions that target that cause (and that’s actually encouraging). Understanding what’s happening on your scalp is the first step toward doing something useful about it.
I suffer from this too. Some weeks are better than others. But knowing the mechanism (knowing it’s not about cleanliness or laziness) makes it a lot easier to deal with calmly.
References
- DeAngelis et al., “Malassezia globosa and restricta: Breakthrough Understanding of the Etiology and Treatment of Dandruff and Seborrheic Dermatitis through Whole-Genome Analysis.” Journal of Investigative Dermatology Symposium Proceedings, 2007. https://www.jidsponline.org/article/S0022-202X(15)52658-4/fulltext
- Ro & Dawson, “The Role of Sebaceous Gland Activity and Scalp Microfloral Metabolism in the Etiology of Seborrheic Dermatitis and Dandruff.” Journal of Investigative Dermatology Symposium Proceedings, 2005. https://www.sciencedirect.com/article/pii/S0022202X15526146
- Naldi et al., “The Global Prevalence of Seborrheic Dermatitis: A Systematic Review and Meta-Analysis.” JAMA Dermatology, 2024. https://jamanetwork.com/journals/jamadermatology/fullarticle/2820685 | PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC11223058/
- “Global and Regional Burden of Seborrheic Dermatitis: Trends in Incidence and DALYs, 1990–2021.” Clinical, Cosmetic and Investigational Dermatology, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12145784/
- “Seborrheic Dermatitis.” Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/seborrheic-dermatitis/diagnosis-treatment/drc-20352714
- Borda & Wikramanayake, “Seborrheic Dermatitis and Dandruff: A Comprehensive Review.” Journal of Clinical and Investigative Dermatology, 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4852869/
About the author: I’m Dusty Combs. I’ve had dandruff for most of my adult life and started this site to document what I learn: what the research actually says, what treatments I’ve tried, what works and what doesn’t. I’m not a dermatologist or any kind of medical professional. Everything here is based on my own reading and experience. If you’re dealing with something persistent or severe, please see a real doctor.
Last updated: June 2026
Medical disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.